(1) Beyond Type 1 diabetes site: https://beyondtype1.org
(2) Drury, P., Gatling, W. (2005) Diabetes. Your Questions Answered.
(3) McDowell, Joan,Matthews, David,Brown, Florence. (2007) Diabetes: a handbook for the primary healthcare team.
(4) McCance, K., Huether, S., Brashers, V., Rote, N. (2010) Pathophysiology.The Biologic Basis for Disease in Adults and Children.
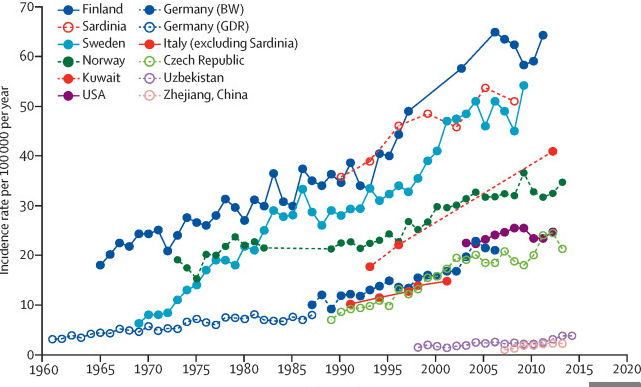
(5) Soltesz, G., Patterson, CC., Dahlquist, G. (2007). Worldwide childhood type 1 diabetes incidence – what can we learn from epidemiology? Pediatric Diabetes.
(6) Diabetes now affects 1 in 10 adults worldwide. IDF site.
(7) Pociot, F., Akolkar, B et al. (2010). Genetics of type 1 diabetes: What’s Next? Diabetes journal. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2889752/
(8) Katsarou, A., Gudbjornsdottir, S., et al. (2017). Type 1 diabetes mellitus. Nature reviews/Disease Primers.
(9) Morran, M., Omenn, G., Pietropaolo, M. (2008). Immunology and Genetics of Type 1 Diabetes. Mount Sinai Journal of Medicine.
(10) Viskari, H., Knip, Mikael., et al (2012). Maternal Enterovirus Infection as a Risk Factor for Type 1 Diabetes in the Exposed Offspring. Diabetes Care. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3357251/
(11) The TEDDY study (The Environmental Determinants of Diabetes in the Young). https://teddy.epi.usf.edu/
(12) Effect of standard nicotinamide in the prevention of type 1 diabetes in first degree relatives of persons with type 1 diabetes by Eduardo Cabrera-Rode et al. In the Autoimmunity paper June 2006.
(13) Karvonen, M., Vilik-Kajander,. Moltchenova, E. et al. (2000). Incidence of childhood Type 1 diabetes worldwide. Diabetes Mondiale (DiaMond) Project. Diabetes Care.
(14) Soltesz, G., Patterson, CC., Dahlquist, G. (2007). Worldwide childhood type 1 diabetes incidence – what can we learn from epidemiology? Pediatric Diabetes.
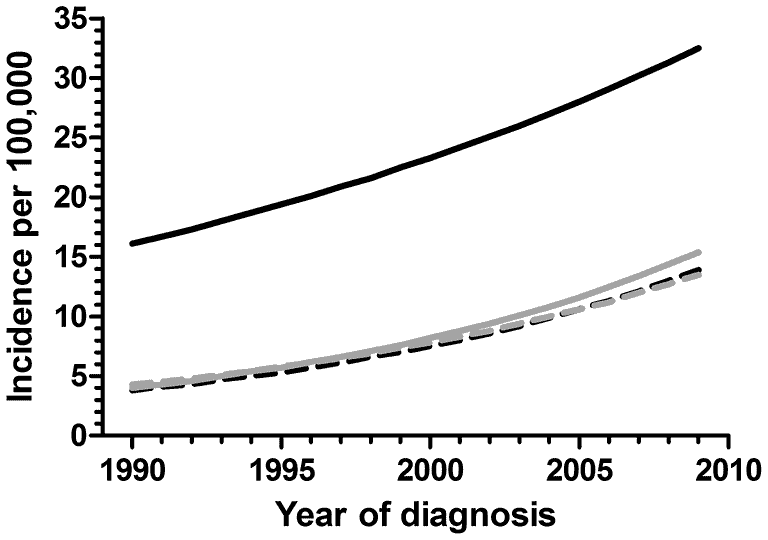
(15) Derraik, J., Reed,P., Jeffries, C., et al. (2012). Increasing Incidence and Age at Diagnosis among Children with Type 1 Diabetes Mellitus over a 20 year Period in Auckland (New Zealand) https://doi.org/10.1371/journal.pone.0032640
(16) Gale, E., Bingley, P., Emmett, C. Collier, T. (2004). European Nicotinamide Diabetes Intervention Trial (ENDIT): a randomized controlled trial of intervention before the onset of Type 1 diabetes.
(17) Von Scholten, Bernt Johan., Kreiner, Frederik., Gough, Stephen., von Herrath, Matthias. (2021). Current and future therapies for Type 1 diabetes. Diabetologia.
(18) Umpierrez, G., Korytkowski, M. (2016). Diabetic emergencies-ketoacidosis, hyperglycemic hyperosmolar state and hypoglycemia. National Review Endocrinology.
(19) McCance, K., Huether, S., Brashers, V., Rote, N. (2010). Pathophysiology. The Biologic Basis for Disease in Adults and Children.