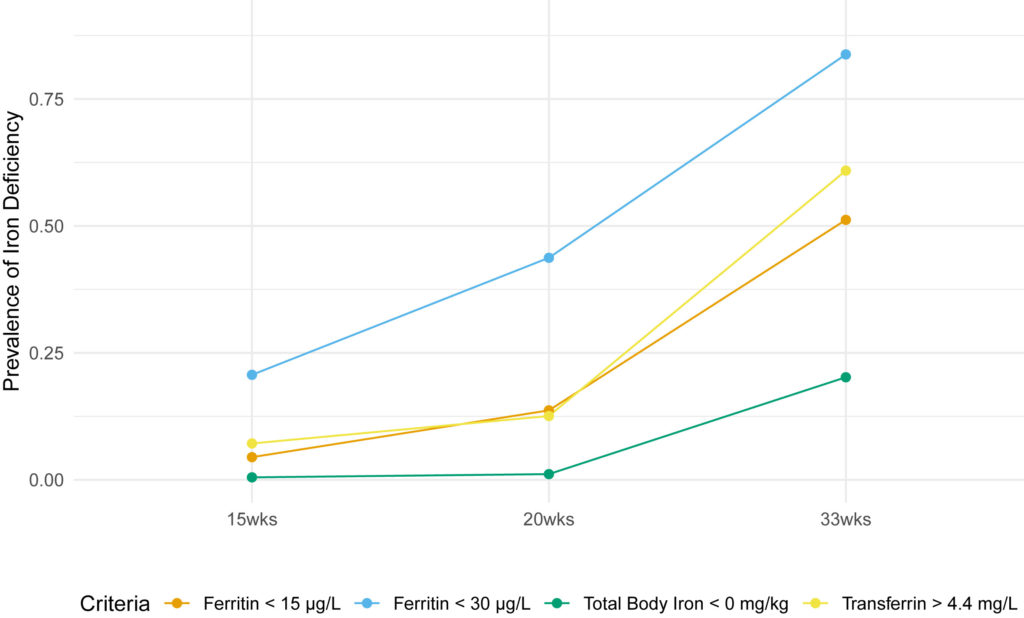
(1) Cochrane, K.M., Hutcheon, J.A., & Karakochuk, C.D. (2022). Iron-deficiency prevalence and supplementation practices among pregnant women: a secondary data analysis from a clinical trial in Vancouver, Canada. The Journal of Nutrition.
(2) Maia, S.B., Souza, A.S.R., Caminha, M.F.C., da Silva, S.L., Cruz, R.S.B.L.C., et al. (2019). Vitamin A And Pregnancy: A Narrative Review. Nutrients. https://www.mdpi.com/2072-6643/11/3/681
(3) Jouanne, M., Oddoux, S., Noël, A., & Voisin-Chiret, A.S. (2021). Nutrient Requirements During Pregnancy And Lactation. Nutrients. https://www.mdpi.com/2072-6643/13/2/692#
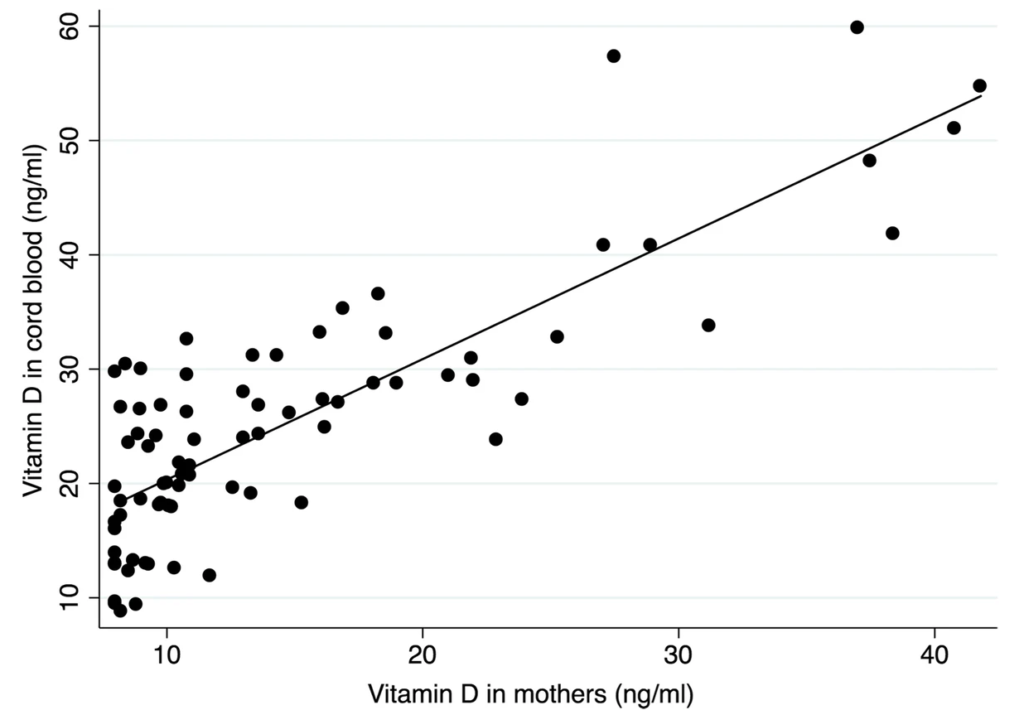
(4) Abdelmageed, R.M., Hussein, S.M.M., Anamangadan, S.M., et al. (2024). Prospective Cohort Study of Vitamin D Deficiency in Pregnancy: Prevalence And Limited Effectiveness of 1000 IU Vitamin D Supplementation. Women’s Health. https://journals.sagepub.com/doi/full/10.1177/17455057231222404
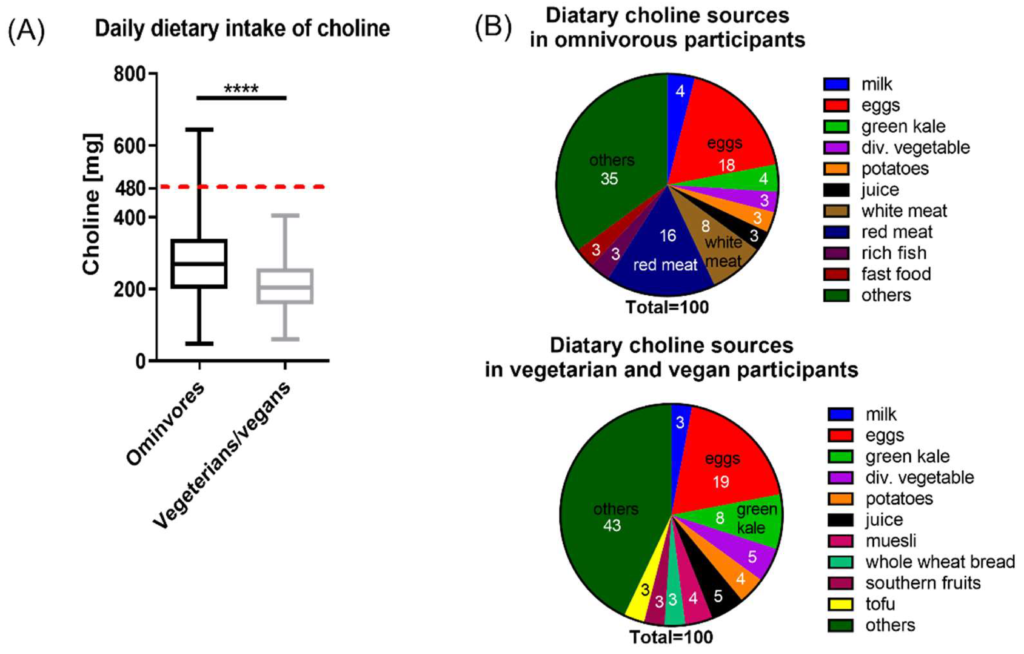
(5) Roeren, M., Kordowski, A., Sina, C., & Smollich, M. (2022). Inadequate Choline Intake in Pregnant Women in Germany. Nutrients. https://journals.sagepub.com/doi/full/10.1177/17455057231222404
(6) Derbyshire, E.J. (2025). Choline in Pregnancy And Lactation: Essential Knowledge for Clinical Practice. Nutrients. https://pmc.ncbi.nlm.nih.gov/articles/PMC12073457/
(7) Lopes, C.A., Prazeres, S., Martinez-de-Oliveira, J., Limbert, E., & Lemos, M.C. (2022). Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey. Nutrients. https://www.mdpi.com/2072-6643/14/7/1393
(8) Mulder, K.A., King, D.J., & Innis, S.M. (2014). Omega-3 Fatty Acid Deficiency in Infants Before Birth Identified Using a Randomized Trial of Maternal DHA Supplementation in Pregnancy. PLoS One. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0083764
(9) Brown, B., & Wright, C. (2020). Safety And Efficacy of Supplements in Pregnancy. Nutrition Reviews. https://academic.oup.com/nutritionreviews/article/78/10/813/5700577
(10) Basak S, Mallick R, Duttaroy AK. Maternal Docosahexaenoic Acid Status during Pregnancy and Its Impact on Infant Neurodevelopment. Nutrients. https://pmc.ncbi.nlm.nih.gov/articles/PMC7759779/