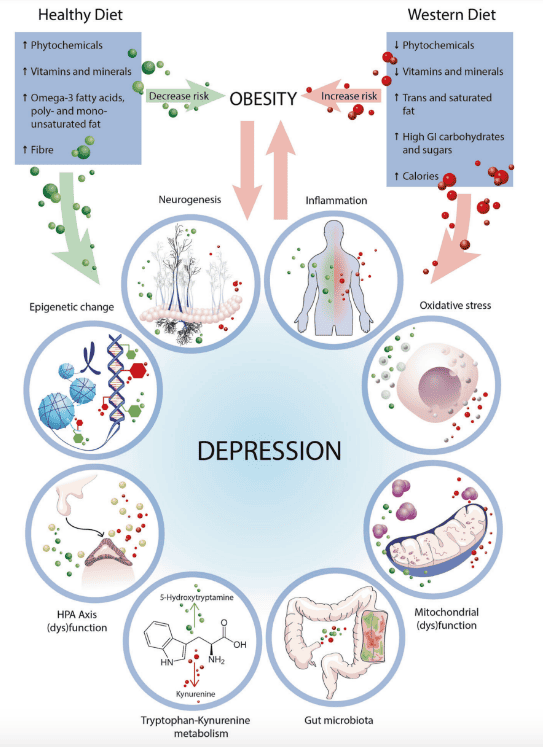
(1) Marx, Wolfgang, Melissa Lane, Meghan Hockey, Hajara Aslam, Michael Berk, Ken Walder, Alessandra Borsini, et al. “Diet and Depression: Exploring the Biological Mechanisms of Action.” Molecular psychiatry 26, no. 1 (2021): 134–150. DOI: 10.1038/s41380-020-00925-x
(2) Vafaei Z, Mokhtari H, Sadooghi Z, Meamar R, Chitsaz A, Moeini M. Malnutrition is associated with depression in rural elderly population. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences. 2013 Mar;18(Suppl 1):S15. PMCID: PMC3743311
(3) Matē, G & Matē, D, The Myth of Normal – Trauma, illness and Healing in a Toxic Culture, Avery, New York, 2023, page 254.
(4) Centres for Disease Control and Prevention, Morbidity and Mortality Weekly Report (MMWR).
(5) Rottenberg, J, The Depths – the Evolutionary Origins of the Depression Epidemic, Basic Books, New York, 2014.
(6) Santomauro, D.F, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Volume 398, ISSUE 10312, P1700-1712, November 06, 202. DOI:https://doi.org/10.1016/S0140-6736(21)02143-7
(7) Sackeim, H, A. et al. Effects of major depression on estimates of intelligence. (2008) Journal of Clinical and Experimental Neuropsychology Pages 268-288. Retrieved from https://www.tandfonline.com/doi/abs/10.1080/01688639208402828
(8) Pratt LA, Druss BG, Manderscheid RW, Walker ER. Excess mortality due to depression and anxiety in the United States: results from a nationally representative survey. Gen Hosp Psychiatry. 2016 Mar-Apr;39:39-45. doi: 10.1016/j.genhosppsych.2015.12.003. Epub 2015 Dec 18. PMID: 26791259; PMCID: PMC5113020. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5113020/
Other bibliography
(1) Hari, J, Lost Connections, Bloomsbury Circus, London, 2018.
(2) Hayes, S, A Liberated Mind, Random House, London, 2019.
(3) Jacobs, M, The Presenting Past – The Core of Psychodynamic Counselling and Therapy, Open University Press, Maidenhead, 2009.
(4) Leader, D, The New Black: Mourning, Melancholia and Depression, Penguin, London, 2008.
(5) Matē, G, When the Body Says No – The Cost of Hidden Stress, Scribe, Victoria, 2022.
(6) Matē, G & Matē, D, The Myth of Normal – Trauma, illness and Healing in a Toxic Culture, Avery, New York, 2023.