(1) McCance, K. L., & Huether, L. E. (2010). Pathophysiology: The biologic basis for disease in adults and children. Mosby.
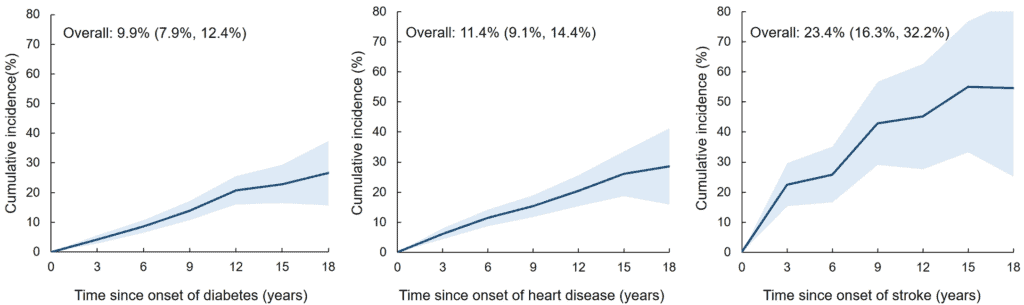
(2) Diabetes UK. (n.d.). Diabetes and stroke. Diabetes UK. Retrieved from https://www.diabetes.org.uk/guide-to-diabetes/complications/stroke
(3) Gonzalez, J. S., Fisher, L., & Polonsky, W. H. (2011). Depression in Diabetes: Have we been missing something important? Diabetes Care, 34(1), 236–239. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3005471/
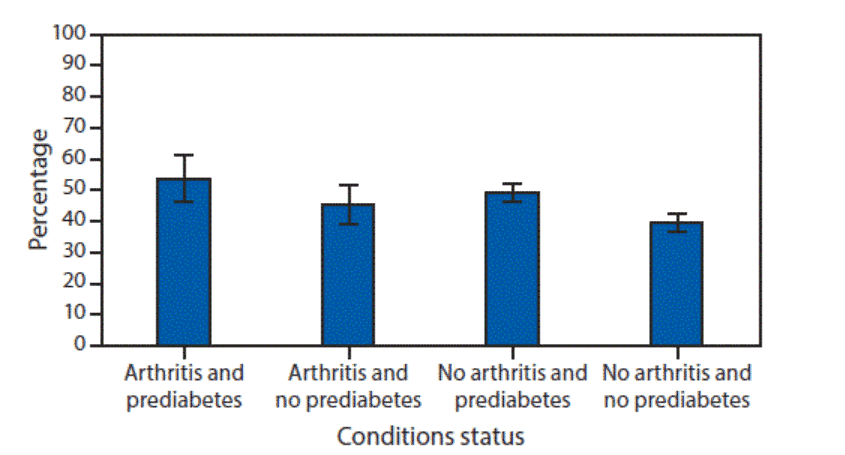
(4) Rath, L. (n.d.). Rheumatoid arthritis and type 2 diabetes. Arthritis Foundation. Retrieved from https://www.arthritis.org/health-wellness/about-arthritis/related-conditions/other-diseases/rheumatoid-arthritis-and-type-2-diabetes
(5) Brown, S. (2004, January). Osteoporosis: An under-appreciated complication of diabetes. Clinical Diabetes, 22(1), 10–20. (2004) Retrieved from https://diabetesjournals.org/clinical/article/22/1/10/1411/Osteoporosis-An-Under-appreciated-Complication-of
(6) Rojas, M., Chávez-Castillo, M., Bautista, J., Ortega, Á., Nava, M., Salazar, J., Díaz-Camargo, E., Medina, O., Rojas-Quintero, J., & Bermúdez, V. (2021). Alzheimer’s disease and type 2 diabetes mellitus: Pathophysiologic and pharmacotherapeutics links. World Journal of Diabetes, 12(6), 745–766. Retrieved from https://doi.org/10.4239/wjd.v12.i6.745
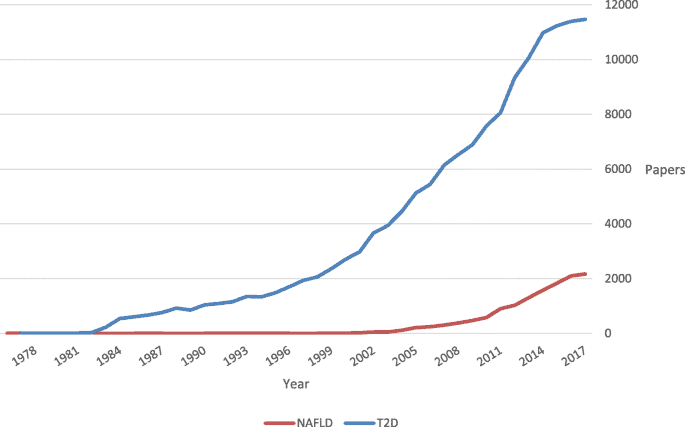
(7) Hazlehurst, J. M., Woods, C., Marjot, T., Cobbold, J. F., & Tomlinson, J. W. (2016). Non-alcoholic fatty liver disease and diabetes. Metabolism: Clinical and Experimental, 65(8), 1096–1108. Retrieved from https://doi.org/10.1016/j.metabol.2016.01.001
(8) Casqueiro, J. , Casqueiro, J., & Alves, C. (2012). Infections in patients with diabetes mellitus: A review of pathogenesis. Indian Journal of Endocrinology and Metabolism, 16(Suppl1), S27–S36. Retrieved from https://doi.org/10.4103/2230-8210.94253
(9) Bader, M. S. (2008). Diabetic foot infection. American Family Physician. 78(1), 71–79. Retrieved from https://www.aafp.org/pubs/afp/issues/2008/0701/p71.html